Racial disparities in breast cancer outcomes remain persistent in the United States. Although Black women have a slightly lower incidence of breast cancer than any other racial or ethnic group, they have a substantially higher mortality rate and are more often diagnosed at younger ages and at advanced stages.
A recent study suggests a historically overlooked contributor: redlining. The study found that patients living in neighborhoods shaped by past housing discrimination had worse breast cancer survival—though the difference narrowed when access to care and treatment factors were accounted for.
Redlining is a 1930s policy that denied insurance and mortgages in predominantly Black neighborhoods, and continues to influence healthcare access today through hospital availability, screening resources, and care continuity.
The findings suggest breast cancer disparities may be driven less by biological differences and more by care delivery conditions, affecting staging at diagnosis, treatment adherence, and ultimately survival.
Redlining refers to discriminatory 1930s housing policies that denied mortgages and insurance in predominantly Black neighborhoods, shaping patterns of residential segregation and economic disparities that still exist today.
Although the policy ended several decades ago, its effects remain evident in the health system. Redlined neighborhoods are more likely to have fewer specialty clinics, limited screening facilities, longer travel distances to cancer centers, and reduced continuity of care.
For cancer patients, these conditions can influence outcomes, with potential for late-stage diagnosis, treatment delays, and incomplete therapy. As a result, redlining functions less as a historical artifact and more as an ongoing structural determinant of health that can affect breast cancer survival.

Associations between historical redlining and breast cancer survival have changed over time, with a narrowing of disparities, according to a study published online Feb. 9 in Cancer.
Sarah M. Lima, Ph.D., M.P.H., from the University of Buffalo in New York, and colleagues examined the associations between historical redlining and all-cause survival of breast cancer from 1995 to 2019. The registry-based cohort included 135,827 patients with breast cancer diagnosed between 1995 and 2019. A historical redlining grade (range A to D) was assigned to cases, which were then divided into five-year diagnostic time periods. The associations with survival were estimated.
The researchers identified a significant time interaction with historical redlining for survival. For grade D versus grade A, survival disparities were largest in 1995 to 1999 and lowest in 2005 to 2009 (hazard ratios 1.75 and 1.48, respectively). For local and regional tumors, redlining associations were largest in 1995 to 1999 and attenuated over time. Among distant tumors, redlining was generally not associated with survival. Among patients with hormone receptor-positive tumors, D-grade versus A-grade survival disparities increased over time. Among all race/ethnicity groups, significant temporal effects were detected.
“Historical redlining continues to have lasting effects on breast cancer mortality today, but our findings show that the effects are not necessarily permanent, and it’s not too late to intervene,” Lima said in a statement.
These findings suggest that breast cancer disparities may be driven less by tumor biology alone and more by the conditions surrounding care delivery. Black patients living in historically under-resourced neighborhoods often encounter barriers that can affect every step of the cancer care journey.
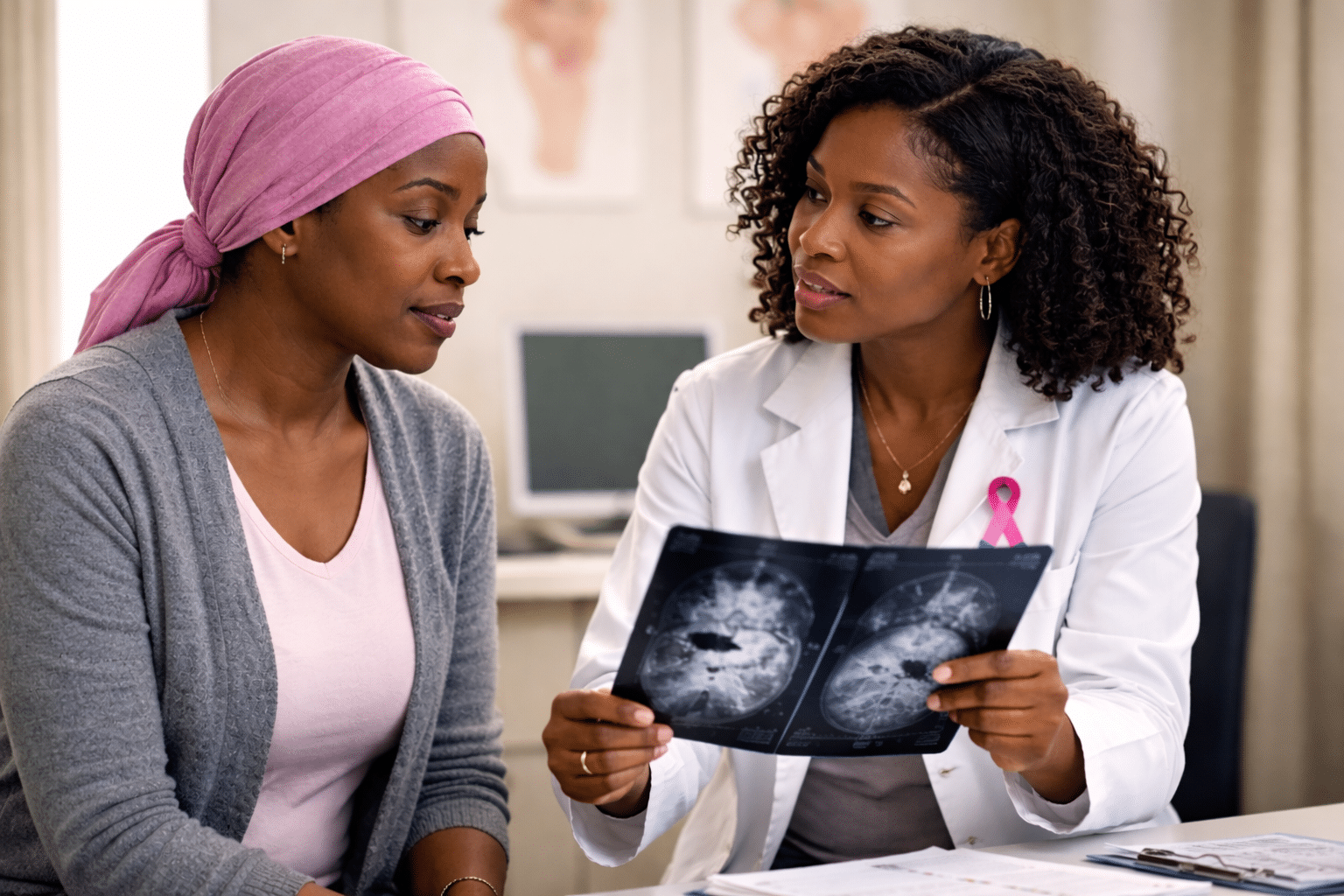
Access to breast cancer screening is one of the earliest points of divergence. Limited availability of nearby imaging centers, transportation challenges, and inflexible work schedules can delay routine mammography, contributing to diagnosis at later stages. Following diagnosis, fragmented referral networks may delay entry into specialty oncology care, and longer travel distances can reduce attendance at medical consultations and follow-up visits.
Treatment completion is another crucial factor. Therapies, such as chemotherapy and radiation therapy, require repeated visits over several weeks or months. Transportation challenges, caregiver responsibilities, or work constraints may lead to missed appointments, resulting in dose reductions or early discontinuation of treatment. These patterns are often labeled as “non-adherence,” yet they frequently reflect structural barriers rather than patient preference.
While structural inequities extend beyond individual practices, clinicians can identify patients at higher risk of treatment disruption and intervene earlier in the care process.
Practical steps can include:

Historical redlining continues to appear in survival statistics, but the new findings suggest the disparities are modifiable–not inevitable. When patients receive timely, consistent care, gaps in outcomes shrink significantly. For clinicians, this shifts disparities from
By subscribing, you consent to receive emails from BlackDoctor.pro You may unsubscribe at any time. Privacy Policy & Terms of Service.
Are you a healthcare professional? Register with us today!